Hi, Everyone,
As promised, I am following up on the email I sent a couple of weeks ago examining the risks and benefits of vaccinating healthy children and young adults against Covid-19.
Today, I’d like to focus on the 5- to 11-year-old age group. In particular, I’d like to answer the question, “Is there any scientific basis for a vaccine mandate for 5- to 11-year-olds?”
This is a critical question because as we speak, school districts across the U.S. (and the world) are beginning to require Covid vaccines for kids as a condition for attending school. Excluding children from in-person education is a dramatic and unprecedented step to take, so the bar for evidence to support a decision with such far-reaching consequences should be very high.
In this email, I will argue that not only has this high bar not been met, but there is also no evidence whatsoever to support a vaccine mandate for 5- to 11-year-old kids, and such a mandate is both unscientific and immoral.
Specifically, I will show that:
- Covid was already a very mild illness for healthy children, and the Omicron variant looks to be even milder.
- Kids 5 to 11 years old have never been significant spreaders of SARS-CoV-2 (to other children or adults).
- Covid infection in kids produces far more robust and long-lasting immunity than the vaccines.
- More than half of kids in the U.S. (and likely other industrialized countries) have already had Covid-19, and vaccinating kids with natural immunity doesn’t provide additional protection.
- There is no direct evidence that vaccines reduce severe illness, hospitalization, or death in 5- to 11-year-old kids. This is even more true with Omicron.
- The Covid vaccines do not prevent transmission of the virus (especially with the Omicron variant).
- There is already concerning evidence of harm from the vaccines in 5- to 11-year-old kids—and the long-term effects are unknown.
- The mandates will cause serious and lasting harm to unvaccinated children.
This will be a long email. I considered splitting it into parts, but I wanted to present the entire case in one place so you can more easily refer back to it and share it with others.
So, grab a cup of tea, and get comfortable!
[Author’s note: the question of whether Covid vaccine mandates make sense for any age group is also worthy of critique, but I want to dedicate this email to 5- to 11-year-old children for reasons that will become clear shortly.]
#1: Covid was already a very mild illness for healthy children, and Omicron looks to be even milder
We’ve known since the beginning of the pandemic that the vast majority of Covid-19 cases in healthy children 5 to 11 years old are extremely mild.
According to the Centers for Disease Control and Prevention (CDC), there have been just 216 deaths in this age group since the start of the pandemic. This represents only 0.03% of the total Covid-19 deaths, despite the fact that 5- to 11-year-old kids comprise almost 9% of the population.

With 28,384,878 kids in this age group, that’s a mortality rate of 0.0008%. Put another way, at worst, a child 5 to 11 years old has a 1 in 131,411 chance of dying from Covid-19.
But even this very low number is likely to be a significant overestimate for healthy children for two reasons.
The first is that Covid deaths have almost certainly been over-counted in the U.S. and other industrialized countries because of how they are classified. For example, say a child with a pre-existing leukemia diagnosis is admitted to the hospital for issues related to their disease. The child tests positive for SARS-CoV-2 upon admission, does not develop any signs or symptoms of Covid-19 infection, but later dies due to complications of leukemia. This will be classified as a Covid-19 death—even though, in this case, Covid-19 likely had nothing to do with the child’s passing.
The overestimate of hospitalizations and deaths due to this method of classification is not small. A recent analysis out of the U.K. found that a full two-thirds of patients with Covid-19 in the hospital only tested positive AFTER being admitted for another condition.
The second reason is that the majority of hospitalizations and deaths in 5- to 11-year-olds occur in children with pre-existing health conditions. A study by the CDC back in September 2020 found that, among 121 childhood deaths related to Covid-19, 75% had an underlying health condition. Another study by the CDC found that 53% of kids hospitalized for Covid-19 had at least one pre-existing condition, the most common being obesity (45%), asthma (14%), and neurological conditions (13%). Yet another large, international review of 14 studies covering almost 20,000 children found that kids with pre-existing conditions were over 25 times more likely to experience severe symptoms from Covid-19 infection than healthy kids.
The point here is not that kids with pre-existing conditions don’t deserve our consideration. Of course they do! The question I am trying to answer in this email is whether the vaccines should be mandated for all 5- to 11-year-old children, including healthy ones. And to do that properly, we have to know what the risk is for healthy children specifically.
Unfortunately, the CDC does not routinely distinguish between healthy kids and kids with pre-existing conditions in their reporting of Covid-19 hospitalizations and deaths. But some other industrialized countries do.
For example, a recent study out of Germany looked at just over 400,000 healthy 5- to 11-year-old kids with no pre-existing conditions who tested positive for Covid-19. They found:
- A rate of hospitalization of 8.5 per 100,000 (~1 in 11,750)
- A rate of ICU admission of 2 per 100,000 (1 in 50,000)
- A rate of death of ZERO (there was not a single death in this age group)
This gives us a much better idea of what we can expect in terms of the risk of hospitalization and death in healthy kids in this age group.
Omicron appears to be milder than previous variants
That said, even these incredibly low numbers are related to previous variants of Covid-19, like Alpha, Beta, and, most recently, Delta. But the Omicron variant has already become dominant for new cases in many countries like South Africa, Denmark, the U.K., and the U.S.
And all of the early data we have so far suggest that Omicron is far milder than all previous variants.
Denmark has been producing very detailed daily reports of Covid cases and hospitalizations throughout December. According to their most recent report from December 24, there have been 27,132 Omicron cases so far, but there have been only 35 Omicron-related hospitalizations. This is a hospitalization rate of 0.13%—which is approximately 8-fold lower than the estimated hospitalization rate for Delta (~1%).
It’s also worth pointing out that there have been fewer than 5 ICU admissions from Omicron. Denmark doesn’t report on the exact number, so, for all we know, it could be zero. Or, it could be 4. Either way, it’s an incredibly small number given almost 30,000 cases.
There’s more to say about Omicron, and I’ll be writing a separate email about that soon. For now, it’s enough to say that if the current trends hold, we should expect the risk of hospitalization and death from Covid-19 in healthy children—which is already incredibly low—to be lower still in the future.
When we consider that:
- Covid-19 was already an extremely mild illness for healthy kids 5 to 11 years old
- Hospitalizations and deaths have been over-counted
- Omicron appears to be far milder than previous variants
… we get a current risk of serious outcomes like ICU admission or death in healthy 5- to 11-year-old kids that is minuscule.
#2 Kids have never been significant spreaders of SARS-CoV-2 (to other children or adults)
Some advocates of vaccine mandates have argued that, while Covid-19 is a mild illness in kids, we should vaccinate them anyway in order to protect those at the highest risk, like the elderly and individuals with pre-existing conditions.
In order for this argument to be valid, two things would need to be true:
- We’d need evidence of significant child-to-adult and child-to-child transmission of Covid-19.
- We’d need evidence that the vaccines prevent, or at least significantly reduce, the transmission of SARS-CoV-2.
In fact, neither of those is the case.
Studies have now shown that kids under 10 years old rarely transmit Covid-19, and all kids/adolescents up to 20 years old are only 43% as susceptible to the disease and 63% as likely to infect others than adults.
I will address the question of whether the vaccines prevent or reduce transmission in detail below, in section #5. The short answer is: they don’t.
Given that neither of these things is true, the argument that we should vaccinate kids to protect the vulnerable has no scientific basis.
#3: Covid infection in kids produces far more robust and long-lasting immunity than the vaccines
Another argument I’ve heard to justify a massive vaccination campaign for 5- to 11-year-old kids is that the vaccines provide more robust immunity than a natural infection and that because of this, the vaccines will “end the pandemic.”
Numerous studies have now shown that this is not the case, and, in fact, the opposite is true: kids who have a Covid-19 infection go on to develop much stronger, more lasting, and broader immunity against future SARS-CoV-2.
A new, peer-reviewed study published in Nature Immunology on December 22 found that both the innate (initial antibody response) and adaptive (later T-cell response) immune reaction to SARS-CoV-2 is much stronger in children than in adults.
In other words, kids who get Covid-19 mount a more effective and robust immune response to the disease than adults do. What’s more, this immune response lasted throughout the entire length of the study period—which was nearly one year—and it appeared to protect them against multiple SARS-CoV-2 variants.
The authors speculate that increased immunity to coronaviruses that cause the common cold, and are cross-reactive with SARS-CoV-2, may be part of the reason that children are more protected from Covid-19 than adults.
From the study:
“In conclusion, we showed that children display a characteristically robust and sustained adaptive immune response against SARS-CoV-2 with substantial cross-reactivity against other hCoVs [human coronaviruses].”
Given how remarkably low the risk of serious illness is in 5- to 11-year-old kids, and given how strong and long-lasting their immune response is to natural infection, wouldn’t it make more sense to simply allow healthy kids in this age group to get Covid-19—especially now that the Omicron variant is becoming dominant—rather than expose them to vaccines with uncertain benefits and concerning side effects (more on both of these points below)?
#4: More than half of kids in the U.S. (and likely other industrialized countries) have already had Covid-19
At the end of May of this year, the CDC estimated that 36% of all children had been infected with SARS-CoV-2. That estimate was made 16 months into the pandemic. If we adjust that estimate for the current time frame (22 months), we get 49.8% or roughly half of U.S. children.
However, the CDC estimate was performed before the emergence of the Delta and Omicron variants, both of which are significantly more transmissible than prior variants. Therefore, it is highly likely that the rate at which kids were getting infected between May 2021 and now is significantly higher than during the first 16 months of the pandemic. This means that more than half of U.S. children have natural immunity against Covid-19.
The Nature Immunology paper I just mentioned above clearly indicates that natural immunity to Covid-19 is especially robust in children.
We also have other evidence that natural immunity is stronger than vaccine-induced immunity. For example, previous research out of Israel suggested that those who had recovered from Covid-19 infection were 13 times less likely to be reinfected than those who’d been vaccinated but had not yet had Covid-19.
And so far, there is little convincing evidence that vaccinating someone who has already been infected offers any benefit.
For example, a study published in June 2021 by Cleveland Clinic of almost 53,000 people found that vaccinating people with natural immunity (i.e., those who had already been infected with SARS-CoV-2) did not confer additional protection. Most importantly, there was not a single case of reinfection among the 1,359 previously infected, unvaccinated subjects in the study.
The fact that most kids have already had Covid-19 and thus already have immunity to it, and that vaccinating people who’ve already been infected doesn’t strengthen their protection against the virus, casts even further doubt on a universal vaccine campaign for 5- to 11-year-olds.
#5: There is no direct evidence that vaccines reduce severe illness, hospitalization, or death in 5- to 11-year-old kids
When I have a chance to talk to parents about the Covid vaccines for kids, I’ll often ask them what they’ve heard about the effectiveness of the vaccines in kids 5 to 11 years old.
Most will respond by saying that they’ve read that the vaccines are “over 90% effective” for kids in this age group.
They’re often quite surprised—even shocked—to learn that, in fact, we know very little about the potential benefits of these vaccines in kids 5 to 11 years old.
Why? Because severe illness in kids is so rare that there wasn’t a SINGLE case of severe Covid-19 or a SINGLE death from Covid-19 in the 2,268 kids that Pfizer studied to obtain their Emergency Use Authorization (EUA) by the CDC.
Because there were no significant adverse outcomes from Covid-19 in the trial, Pfizer had to estimate the potential benefit by looking at the antibody response generated by the vaccine in the kids’ blood.
There are several problems with this. First, antibodies are a poor predictor of clinical response to Covid-19. Second, since there were no cases of severe Covid-19 in kids in this study, Pfizer had no idea what antibody level would be protective against severe infection.
This means that any claims you’ve seen that the Pfizer vaccine is 90% effective are misleading because this only refers to an antibody response in the blood from the vaccine and not actual protection against severe illness, hospitalization, or death.
Yes, the massive campaign to vaccinate 5- to 11-year-old kids is based on a small study of 2,268 kids in which the vaccines did not prevent a single case of severe Covid-19 or a single death and demonstrated only an elevated antibody response in those that received the vaccine.
As hard as that is to believe, that’s where we are.
#6: The Covid vaccines do not prevent transmission of the virus (especially with the Omicron variant)
Even before the emergence of the Omicron variant, we already knew that the Covid vaccines do not significantly reduce transmission of the virus. Unlike the measles or polio vaccines, they do not provide “sterilizing immunity”—that is, they don’t keep people from getting the virus or spreading it to others.
CDC Director Rochelle Walensky disclosed this back in August 2021 in an interview with Wolf Blitzer on CNN. She said:
“They [the vaccines] continue to work well with ‘Delta’ with regard to severe illness and death, but what they can't do anymore is prevent transmission.” [Emphasis added]
But in countries where Omicron has become the dominant variant, we have even less reason to believe that the vaccines do anything at all to reduce transmission.
According to Denmark’s Covid-19 report from December 24 (mentioned earlier in this email), 92% of confirmed Omicron cases occurred in people who had received either 1, 2, or 3 doses of a Covid vaccine:

We’re seeing similar data out of Ontario, Canada, which has also been issuing detailed reports on cases. You can see in the chart below that, as of late December, the number of Omicron cases per 100,000 people is virtually identical in the unvaccinated, partially vaccinated, and fully vaccinated:

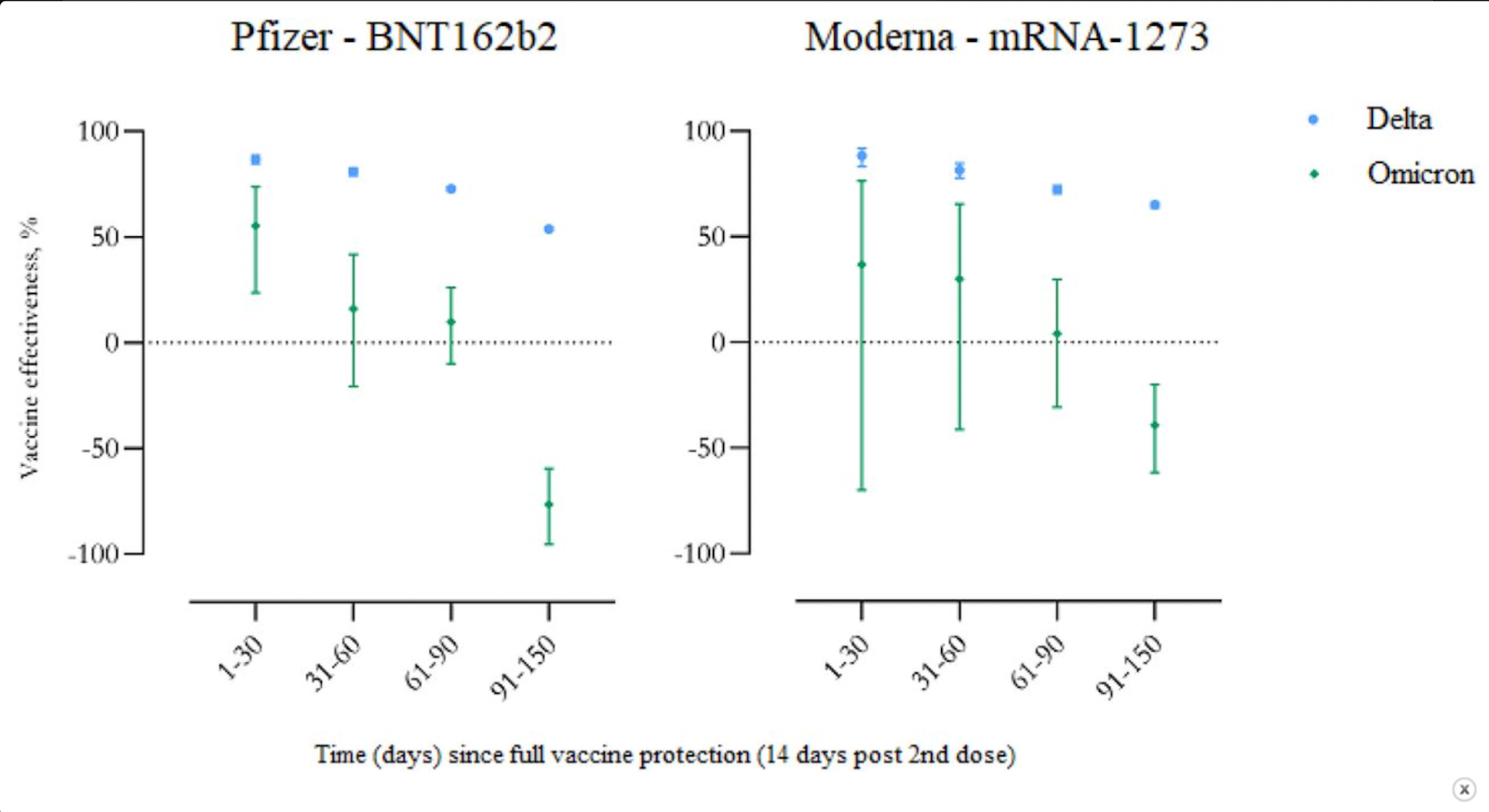
Also, a preprint study out of Denmark shows that vaccine effectiveness against Omicron drops to nearly zero just over two months after peak protection (14 days after the second dose). Even more disturbingly, the vaccines go into negative effectiveness—meaning those who were vaccinated were more likely to contract Covid-19—3 months after peak protection.
Here’s the key figure from that study. The blue dots represent vaccine effectiveness against Delta, and the green dots/bars represent vaccine effectiveness against Omicron. When the dot is above the horizontal line, effectiveness is positive. When it’s below the line, it’s negative.
 Finally, we have data from the U.K.’s “SARS-CoV-2 variants of concern and
Finally, we have data from the U.K.’s “SARS-CoV-2 variants of concern and
variants under investigation in England, Technical briefing 33” indicating that even with a booster, symptomatic protection against Omicron wanes significantly after just 10 weeks:
“Among those who received an AstraZeneca primary course, vaccine effectiveness was around 60% 2 to 4 weeks after either a Pfizer or Moderna booster, then dropped to 35% with a Pfizer booster and 45% with a Moderna booster by 10 weeks after the booster. Among those who received a Pfizer primary course, vaccine effectiveness was around 70% after a Pfizer booster, dropping to 45% after 10-plus weeks and stayed around 70 to 75% after a Moderna booster up to 9 weeks after booster.”
Frankly, these are remarkable data that raise questions about the effectiveness of the current vaccines against Omicron for people of all ages, not just 5- to 11-year-old kids.
It’s clear that we are not in the same situation today that we were in when the vaccines were initially developed. Omicron is very different from Alpha, which was the dominant strain when the vaccines were released. And as these studies clearly show, these vaccines aren’t as effective against Omicron as they were against earlier variants.
At best:
- Two shots of Pfizer provide just over 50% effectiveness for about a month; that drops close to zero just after the second month and goes deeply negative before the third month.
- Two shots of Moderna provide just under 50% effectiveness for about two months; that drops to zero in the third month, and into negative territory shortly after that
- A booster provides an additional 2.5 months of partial protection (below 45% for all but people who received two shots of Pfizer plus a Moderna booster).
If we were starting out with the current vaccines today, with Omicron, that’s the level of protection they would provide. We’d have to start giving boosters just 2–3 months after the initial shots and then give a booster every 2–3 months after that. Does that make sense, given how mild Omicron is for healthy kids (and most adults)?
It’s worth noting that most of these data regarding Omicron infections and vaccination status are from adults, not children, because the vaccines have only recently been offered to 5- to 11-year-old kids. But there is no reason to believe that vaccines will be more effective against Omicron in children than they are in adults (and, in fact, there are reasons to believe they would be less effective, as I’ve described earlier in this email).
#7: There is already concerning evidence of harm from the vaccines in 5- to 11-year-old kids—and the long-term effects are unknown
Despite the incredibly low risk that Covid-19 poses to healthy children, the fact that over 50% of kids have already had Covid, and that natural immunity is robust and durable, some still might argue that vaccinating children makes sense.
After all, if we can save even one life with the vaccines, shouldn’t we do that?
Certainly, if we knew without a doubt that 1) vaccinating every 5- to 11-year-old child would prevent even a small number of severe illnesses and deaths, and 2) the vaccines were 100% safe and would not cause any adverse events, then this would be a strong argument.
However, we still don’t know that vaccinating children this age actually reduces severe illnesses or deaths. All we know is that the vaccines induce an antibody response.
And we already know that the vaccines are not 100% safe and are producing a significant number of adverse events in children 5 to 11 years old. This should not be surprising. All medical interventions have potential side effects and risks, and the Covid vaccines are no exception.
The CDC’s own data show harm for the vaccines—despite Director Walensky’s denial
According to the CDC’s data, as of December 9, 2021, there have been 3,233 reports of adverse events in kids 5 to 11 years old from the Covid-19 vaccines, including 14 reports of myocarditis (8 of which have already met the CDC criteria for a vaccine-induced myocarditis case).

Yet, strangely, Director Walensky went on ABC News the following day, December 10, and said that there have been no cases of myocarditis seen in kids. How is this possible? Was she not aware of the data her own agency issued just the day before? Or was she lying? Either way, it’s incredibly disturbing.

It’s worth pointing out that myocarditis is only one of several possible side effects that have been observed with the Covid-19 vaccines, which include arthritis, autoimmunity, acute liver and kidney injury, thyroiditis, and more.
It’s also important to know that the Vaccine Adverse Event Reporting System (VAERS) is imperfect, and adverse effects are often underreported. For example, a 2001 study found that less than half of cases of rotavirus vaccine-associated intussusception (severe intestinal disorder) were successfully reported to VAERS. And a 2020 study found that the reporting sensitivity for anaphylaxis (severe allergic reaction) and Guillain–Barré syndrome (severe nerve disorder)—both of which have been seen with the Covid-19 vaccines—ranged from 12%–76%.
There are at least 2 reasons to believe that underreporting of side effects for the Covid-19 vaccines is at least as prevalent as the studies above suggest—and probably more:
- Many doctors and nurses are afraid to report side effects of the vaccines because of the current polarized political climate.
- The vaccine program for 5- to 11-year-olds began only recently, and there’s often a lag time between receiving the vaccines, side effects, and reporting of those side effects.
Nevertheless, let’s be generous and assume that the underreporting of side effects from the Covid-19 vaccines in VAERS is only 0.5, or one-half. This would mean 6,466 adverse events reported from 7,141,428 doses of the vaccine in 5- to 11-year-olds, or a risk of a vaccine-related adverse event of 1 in 1,104.
This compares with (according to the German study I mentioned above) a risk of hospitalization of 1 in 11,750, a risk of ICU admission of 1 in 50,000, and a risk of death of zero from Covid-19 in a sample of 400,000 kids.
To make it as clear as possible: these data suggest that, for healthy kids 5 to 11 years old, there is a much higher risk of an adverse event from the vaccine than there is of preventing a hospitalization, ICU admission, or death from Covid-19.
You might argue, “Well, if those adverse events from the vaccine are mild, what does it matter?” That’s a reasonable question to ask. However, many of the side effects reported to VAERS are in the moderate-to-severe range. Most people won’t bother with the time or hassle required to file a VAERS report if they simply had a sore arm for a couple of days.
OpenVAERS has been diligently reporting on the raw VAERS data throughout the pandemic. According to their website, there have been 983,756 Covid vaccine-related reports submitted to VAERS as of December 17, 2021 across all ages. Within the 5- to 11-year-old age group, these include:
- 2 deaths
- 90 hospitalizations
- 331 urgent care visits
- 772 doctor’s visits
- 2 cases of Bell’s Palsy
- 3 cases of anaphylaxis
These are clearly not mild side effects, and together with the CDC’s data on myocarditis risks, there is enough evidence to warrant concern about both the short- and long-term effects of these vaccines—especially since they are being given to healthy children with their entire lives ahead of them.
In addition to the known risks above, there are also the unknown risks. While mRNA vaccines have been studied for many years, they are new, experimental therapies in humans with no long-term safety data. We simply don’t know the long-term risks of these vaccines.
#8: The mandates will cause serious and lasting harm to unvaccinated children
So far, we’ve focused on the risks and benefits for 5- to 11-year-olds receiving the Covid vaccines.
But if these vaccines are mandated as a condition of attending schools in person, as some districts in the U.S. and abroad have already done, we also must consider the potential harm that children who remain unvaccinated—for any reason—may experience as a result of not being able to go to school.
An unvaccinated child will be punished by withholding in-person education and contact with their peers and teachers. This is a far higher risk than a healthy child faces from contracting Covid-19.
School closures have already caused untold harm to children—some of which may be lifelong. As Dr. Vinay Prasad of UCSF has argued, “school closure was the greatest self-inflicted wound of the pandemic.”
As evidence for this, we’ve seen a disturbing rise in mental and behavioral health issues like anxiety, depression, and obsessive compulsive disorder in children. A study published in March 2021 documented a wide range of harms experienced by children during lockdown (which would be similarly experienced by kids excluded from in-person education because of their vaccination status):
- An increase in stress and neuroinflammation
- Rising rates of anxiety, depression, and psychosis
- Weight gain and poor diet
- Potential long-term effects caused by removal from normal social development context
- Rising social inequalities
- Multiple impacts from lack of play
The list goes on and on. But even studies like this one, which can take months to research and publish, are not documenting the full effects. Public health departments, school counselors, and mental health professionals around the world are reporting deeply disturbing patterns.
For example, in Maryland, according to the Department of Health, almost 20% of children contemplated suicide last year, and drug use has increased considerably:

This is a terrifying and horrific statistic that should be sounding the alarms on the impact of keeping kids away from school and isolating them from their peers and other important people in their lives.
We’ve also seen disturbing examples of unvaccinated children being shamed and forced to justify their status in front of the class—a disgusting and scientifically baseless (as you now know) tactic designed to force them into compliance:

Is this the world that we want to live in, where parents are forced to decide between giving their children an unnecessary, ineffective, untested, and unsafe vaccine with both known and unknown adverse effects, so the kids can continue to participate in a normal, healthy life, or not give their kids the vaccine and remove them from many if not most of their typical activities, including attending school in person, eating out at a restaurant, or playing on a sports team?
We do not have to take this path.
Other countries have chosen not to. For example, the U.K.’s expert body the Joint Committee on Vaccination and Immunisation (JCVI) has decided not to vaccinate healthy 5- to 11-year-old children (though they did approve vaccination for kids in this age group with underlying health conditions).
Even if we decided to make the vaccines available for healthy kids in this age group—which I don’t think is an evidence-based decision, for the reasons I’ve laid out above—there’s absolutely no basis for making them mandatory.
- They do not prevent transmission, especially with Omicron.
- There is no direct evidence that they reduce the risk of hospitalization or death.
- The risk of serious illness in healthy kids is extremely low (and likely even lower with Omicron).
- Over half of kids have already had Covid-19 and have robust and lasting immunity. There is no evidence that vaccinating kids with natural immunity provides additional protection.
- There is already evidence of harm from the vaccines.
As parents and caregivers, we have a moral and ethical obligation to safeguard the health and well-being of our children. Mandating the Covid vaccines for 5- to 11-year-olds not only fails to achieve this goal, but it works directly against it in numerous ways.
I believe that once the facts I’ve outlined in this article become more widely known, mandating the Covid vaccines for kids will be viewed as one of the most egregious and unconscionable failures of public health in the history of humanity.
That is why I wrote this email. I want those of you who are parents to truly have informed consent—which is the process by which a healthcare provider educates a patient about the risks, benefits, and alternatives of a given procedure or intervention.
It should be the job of our public health authorities to provide this informed consent regarding the vaccines for 5- to 11-year-olds (and other age groups, as well). Unfortunately, our agencies and authorities are no longer fulfilling their vital role. (As a side note, this shouldn’t surprise my long-time readers. I’ve been writing about the regulatory capture of public health agencies in other contexts for many years. See here and here for examples.)
I know that many of you as parents are finding yourselves in extremely difficult situations, where you feel pressured into giving your children a vaccine that you don’t believe is necessary, just so your kids can continue to participate in normal life.
It’s up to us, as informed citizens, to fight back against these unscientific and immoral mandates, and protect the health and well-being of our children.
There is no duty that is more sacred.
In health,
Chris